First book to describe what pain means in vulnerable or special groups of people
Clinical applications described in each chapter
Provides insight into the nature of pain experience across the lifespan
This book, the third and final volume in the Meaning of Pain series, describes what pain means to people with pain in “vulnerable” groups, and how meaning changes pain – and them – over time.
Immediate pain warns of harm or injury to the person with pain. If pain persists over time, more complex meanings can become interwoven with this primitive meaning of threat. These cognitive meanings include thoughts and anxiety about the adverse consequences of pain. Such meanings can nourish existential sufferings, which are more about the person than the pain, such as loss, loneliness, or despair.
Although chronic pain can affect anyone, there are some groups of people for whom particular clinical support and understanding is urgently needed. This applies to “vulnerable” or “special” groups of people, and to the question of what pain means to them. These groups include children, women, older adults, veterans, addicts, people with mental health problems, homeless people, or people in rural or indigenous communities. Several chapters in the book focus on the lived experience of pain in vulnerable adults, including black older adults in the US, rural Nigerians, US veterans, and adults with acquired brain injury. The question of what pain experience could mean in the defenceless fetus, neonate, pre-term baby, and child, is examined in depth across three contributions.
This book series aspires to create a vocabulary on the “meanings of pain” and a clinical framework with which to use it. It is hoped that the series stimulates self-reflection about the role of meaning in optimal pain management.
Meanings of Pain is intended for people with pain, family members or caregivers of people with pain, clinicians, researchers, advocates, and policy makers. Volume I was published in 2016; Volume II in 2019.
Request a sample by emailing me: simon.vanrysewyk@utas.edu.au, or vanrysewyk@hotmail.com
Buy the complete book on Springer’s website, here.
On the Facebook group, Exploring Pain: Research and Meaning, Phil Greenfield writes: “Pain is a subjective experience, with (in the absence of actual tissue damage) pretty much zero in the way of objectively measurable correlative features, so if we’re aiming to help someone who’s in pain, our focus should rest entirely on helping them with regard to their experience, not with regard to pain.
Am I missing something?”
My response was: The experience of pain is important for the person with pain, but meaningless to other people unless there are observable behaviours. The experience of pain is neither reducible to, nor totally separable from, its associated behaviours.
Suppose we encountered a society of people who used a word that lacked any connection with pain-related behaviour, and the complex situations in which we show it. Would we translate this word as “pain”? It is the meaning assigned to the complex pattern of behavioural responses, nonverbal and verbal, and its circumstances, that motivates attempts to help the person with pain.
Each person we encounter in the world is a unique perspective that is not the body, but the “self”, which is lodged in the face.
“Thousands of photographs from the heart of China’s highly secretive system of mass incarceration in Xinjiang, as well as a shoot-to-kill policy for those who try to escape, are among a huge cache of data hacked from police computer servers in the region.
The Xinjiang Police Files, as they’re being called, were passed to the BBC earlier this year. After a months-long effort to investigate and authenticate them, they can be shown to offer significant new insights into the internment of the region’s Uyghurs and other Turkic minorities.”
An assumption held by some philosophers and scientists is that a person is identical with his or her body. Person and body are one and the same thing.
In terms of our personal experiences, however, this claimed identity between person and body escapes our conscious understanding. For example, when I feel a pain, there is no information or evidence about my body, that could show it to be false. Through my personal experience alone, when I feel a pain, I simply am in pain.
In person-to-person interactions, we respond to each other as though we are not identical with the human body, but in an important sense operating “through” the body, which seems to be a vehicle of thought, emotion, or sensation.
We feel that each person we encounter in the world is a unique perspective that is not the body, but the “self”, which is lodged in the face.
The actions revealed in the face are more meaningful than in other body-parts. This is because body-parts do not have the individuating meaning of the face: the meaning of revealing me, here, now. When I observe another’s pain facial expression, I am not perceiving a physical part of him or her, as I am when I notice his or her injured arm or leg. I am meeting him or her, a real person, who reveals himself in the face.
As a person, I can recognise within myself a perspective or point of view on the world and identify it as belonging to me. Every person has such a unique perspective; this is partly what it means to be a person rather than a physical thing. The computer that I am typing on does not have a personal point of view. It is just a physical thing. It also completely lacks linguistic capacity: it cannot spontaneously use words like “I”, “here”, or “now”. Whenever we use the word “I”, we are describing our point of view about something.
When we “give of our possessions”, as Kahlil Gibran describes, the focus of the giving act lies on the possession, which is a mere thing. It is deficient in having a perspective or point of view on the world partly because it lacks a face. The act of giving mediated by the exchange of a possession is robbed of an essential dimension of shared perspectives, or empathy, which can only be gifted when two people interact face-to-face, person-to-person. Thus, “it is when you give of yourself that you truly give”.
FACE Summit 2022 will take place on May 21, 2022, online and live (School of Face ZOOM Platform), with lectures in English, Spanish and Portuguese. Keynote speakers are exclusive guests of the organizing committee.
The FACE Summit is a registered event from the original idea by Dr. Freitas-Magalhães, PhD, and organized by F-MGI and FEELab/UFP. The FACE Summit motto is “the face is our emotion”. More info: face@facesummit.pt #facesummit2022
Gordon, also known as “Whipped Peter”, a former enslaved African American man, shows his scarred back at a medical examination, Baton Rouge, Louisiana, on 2nd April, 1863. The scars were the result of whipping during his time as an enslaved person at a Louisiana plantation. (Source: Wikimedia Commons)
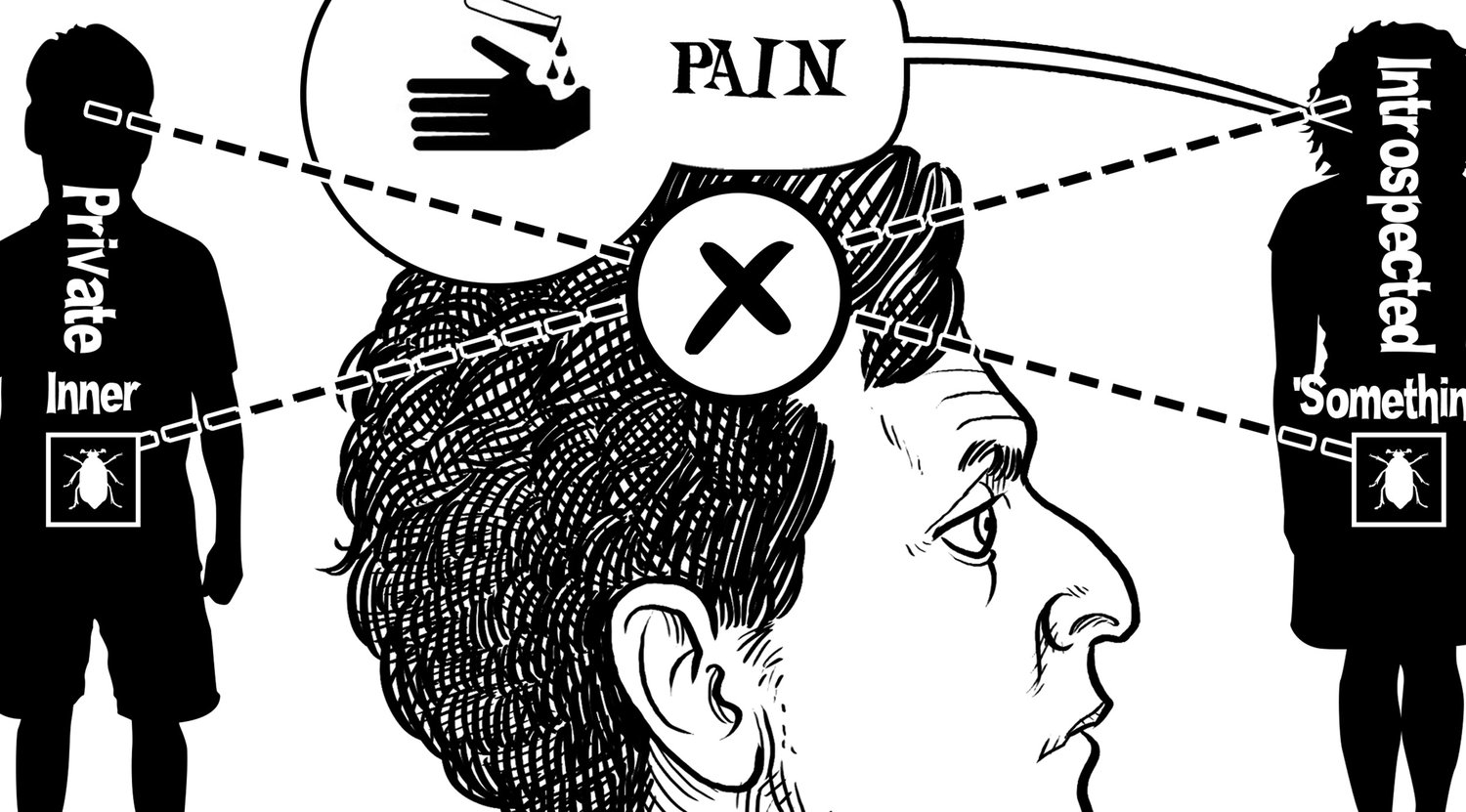
A reason for thinking that pain is private – hidden to external observers – is the uncertainty that affects our judgements about the pain of others.
When someone appears to be in pain, it seems self evident that what matters is not the pain behaviour that we observe, but the pain experience that lies ‘behind’ the behaviour. We find it natural to say that ‘pain is private; we infer it only inconclusively from the behaviour.’
We naturally think: first-person experience is certain; third-person observation is uncertain. The person in pain has privileged, or immediate, access to his or her pain. Doubt is excluded in the first-person case.
Is this thinking correct?
Following the philosopher Wittgenstein, doubt in the first-person is excluded, not because pain is a private experience, but because the practice of pain excludes it. In the practice of pain, the individual has the role of expressing pain experiences; these expressions include a diverse range of verbal and non-verbal behaviours. In the swing and play of the practice, we treat these behaviours as authentic. To introduce doubt here would alter the practice of pain; importantly, it would undermine our concept of the person.
In clinical settings, this is reflected in McCaffery’s maxim that “Pain is what the person says it is, and exists whenever he or she says it does.” This brings the person to the fore, and makes patients the authority in their pain experience. This approach to pain assessment is also aligned with the principles of patient advocacy and ethical clinical treatment.
Why can’t a person be wrong about his or her own pain? The reason Wittgenstein proposed is that assigning the individual the role of expressing pain means there is no gap between what the person sincerely says her experience is, and what it really is. If we are trying to determine the effect of pain on a person’s quality of life, it is what the person says, and not anyone else, that is correct.
The point is not that the individual feels pain only she can feel, but that we treat her as a person, and on the basis of her behaviours, including self-report, assign to her particular sensations, thoughts, and moods. The ‘privacy of pain’ reflects not the intrinsic privacy of pain experience, but our practice of pain based on the notion of a person whose behaviours are treated as authentic expressions of pain.
Still, a person’s utterances may only partly signify the complexities of pain experience, and some situations warrant people be careful what they reveal. Some pain behaviour may therefore reflect perceived best interests, and this is contextual. Care-delivery in pain settings can involve a threat to the caregiver, and is conditional on the authenticity of pain behaviour. As observers of pain behaviour, we are sensitive to signs of exaggeration, suppression, or malingering. Thus, fine shades of behaviour are important in the evaluation of ‘what is going on’ in the setting of pain, and lead our relation to each other as persons. The practice of pain does not always connect behaviour and pain experience in a rigid way.
Navigating these complexities can make patient-clinician interactions challenging.
Illness is definite enough for us to see patterns in it. For example, frequent and severe pain often leads to help-seeking behaviours. But, it is not so definite to be describable in terms of fixed or rigid rules. If we do describe illness in terms of patterns, these must be sufficiently flexible to encompass a degree of indefiniteness – frequent and severe pain does not always lead to help-seeking behaviours.
This indefiniteness is important for human beings, as it allows for variations in our reactions to each other, and to what is happening within each person. Our reactions to others and to ourselves are not uniform, and often rely on context.
Imagine a people who articulated illness in terms of fixed rules; the behaviour of such a people would form simple patterns. Suppose,
The people maintain that the ill person always continues normal social roles the person takes for the duration of the illness
Normal role performance and responsibilities are continued so that the ill person can ‘battle through them’
The strength of this continuation never varies directly with the severity of the illness
The lives of such a people would be very different from our own, and how we would relate to them is unclear. A concept of illness governed by definite rules would be unable to cope with the variation, which for us, is the essence of life itself.
Parallel to the indefiniteness of the concept ‘illness’ in everyday life, is the indefiniteness of the diagnostic process. Physicians slowly move toward closure of diagnostic possibilities through testing and analysis, and through a ‘rule-out’ mentality, which may lead to a diagnosis. Diagnosis is uncertain. There are no fixed rules in medicine stipulating what counts as sufficient information to make a diagnosis. This overlaps with the uncertainty that characterises our judgements about what others are thinking, feeling, and experiencing.
By its nature, diagnosing illness is about managing indefiniteness: it attempts to reduce the level of diagnostic uncertainty enough to make optimal therapeutic decisions.
Intolerance to diagnostic uncertainty has negative implications in general practice, on patients, and the healthcare system. General practitioners who cope well with uncertainty are more likely to support shared decision-making. By attempting to achieve absolute certainty through a ‘correct diagnosis’, premature closure may occur in the decision-making process, thereby allowing hidden assumptions and unconscious biases to have more weight than they should, with increased potential for diagnostic error.
The indefiniteness of illness does not reflect the inadequacy of our language, but the complexity that characterises human life.
The debate is not substantive or of practical import. It does not involve disagreements about pain physiology, what causes pain, or how pain should be treated. Instead, the debate is semantic.
The debate is easily resolved by simply looking at textbooks that describe how the terms sensation and perception are conventionally defined and used.
These textbooks make clear that it is completely appropriate to refer to pain as a perception, and it doesn’t make much sense to say that pain is a sensation but not a perception.
In any event, it doesn’t matter that much how we use these words in practice, because they are inherently fuzzy and often used interchangeably.
I think Todd’s post is a decent contribution to the question, and will make a positive difference to some patients and HCPs.
Below, some thoughts from me; Todd, if you read this, your response is very welcome.
Todd: “…the terms sensation and perception are inherently nebulous and there’s no bright line between them. Why not? Because they encompass a vast number of different physiological processes happening at every level of the nervous system…”
Me: The terms ‘sensation’ and ‘perception’ are ordinary language terms, and do not capture neurophysiological or genetic differences, but differences in the kinds of behavioural and perceptual capacities human beings are interested in. We are social by nature. Human languages include psychological terms because of our need to describe, explain, predict, and otherwise understand the behaviour of other human (and non-human) animals, and because of the need to provide such information to other humans.
Of course, psychological terms can be defined or characterised scientifically, but the original ‘home’ of our psychological vocabulary is the ordinary language we use every day.
Todd highlighted the indeterminacy of our psychological terms, such as ‘sensation’ and ‘perception’; e.g., ‘…there’s no bright line between them’; ‘…are inherently fuzzy, and are often used interchangeably’.
Me: I think the possibility of disagreement or uncertainty about pain in others reflects this indeterminacy. In our ordinary pain language, that indeterminacy is not due to neurophysiological or genetic factors, but to social patterns of behaviour: our concept of pain is flexible because pain behaviour, and our complex reactions to it, is diverse and unpredictable. Care-giving in pain settings can involve a threat to the caregiver, and is conditional on the authenticity of manifest pain behaviour. As observers of pain behaviour, we are sensitive to signs of exaggeration, suppression, or malingering, in behavioural displays of pain. Accordingly, our concept of pain does not always connect behaviour, situation, and personal experience, in a rigid way.
What could follow if we always connected behaviour, situation, and personal experience, in a rigid – necessary – way? To propose a simple, but rather extreme, illustration: suppose a group of people defined pain in terms of a particular neurophysiological biomarker, and used a sophisticated scanner to test for this marker. In their practice, the scanner’s verdict, and not the individual’s utterances or behaviour, is treated as definitive.
Would we want to call this practice a concept of pain? Would this practice be desirable or even possible for us? Would we, for example, accept that an apparent malingerer was in pain, if the scanner said so? Or, that a friend wasn’t, despite her facial grimaces? Would the absence of an abnormal scanner finding be held against a person applying for health benefits?
The new practice with its unanimity and clarity would be a far cry from our current, indeterminant, one. Although some people might engage in this practice, the fact that they do so perhaps makes them a different type of people from us?
How do children learn the concept of pain? What is the ‘concept of pain’?
Children’s pain language
“Children rapidly develop an extensive vocabulary to describe pain between 12 and 30 months of age, with words for pain from injury emerging first and reflecting the development of normal speech acquisition. The differences in verbal expressions in the context of minor illnesses and injuries suggest that children make a cognitive distinction between the origins and sensory aspects of pain.
“Children’s expressive pain vocabulary appears to serve multiple purposes beyond simple description.We found that very young children have awareness of objects and actions that can alleviate pain and use language to seek parents’ attention and to engage parents in pain relief activities. In keeping with general language development, the youngest children used individual pain words or exclamations to convey more complex concepts (known as holographic or telegraphic speech) whereas older children demonstrated greater linguistic competence, including use of metaphor, simile and analogy (Karmiloff & Karmiloff-Smith 2001; Meadows 2006). Interestingly, the basic exclamatory vocalizations are retained throughout childhood and may reflect familial or cultural context that persist into adulthood (Craig et al. 2006).We found that parents’ communicative intent was primarily to gain further information from children about the source and nature of pain and to direct children’s behaviour.”
Franck L, Noble G, Liossi C. From tears to words: the development of language to express pain in young children with everyday minor illnesses and injuries. Child: care, health and development. 2010;36(4):524-33.
“Children’s use of the different pain descriptors changes as they grow older. Younger children (≤3;11), for example, mainly use interjections, such as “ouch” or “ow,” and words like “ache” to describe their pain. Literature indicates that children start to use the word “pain” for the first time at the age of 3;0 to 3;11 (Craig et al., 2006) and continue to use interjections and descriptors to describe their pain as they grow older (Craig et al., 2006; Ely, 1992; Wennström & Bergh, 2008).
When younger children do not yet have the cognitive and language skills to explain the bodily sensations that they experience during pain (Dubois et al., 2008), they try to explain pain with concrete phrases like “I lose my smile and feel bad” (Jerrett & Evans, 1986) or “I’m not feeling well” (Kortesluoma & Nikkonen, 2006). Some use comparisons such as “I had a real bad – kinda like a scar” (Ely, 1992) or “Feels like someone hit it with a sledge hammer” (Abu-Saad, 1984a). Other children explain what caused the accident that resulted in the pain experience, such as “I was playing too rough…” (Harbeck & Peterson, 1992) or “I touched the warm pot” (Johnson et al., 2016).
As children’s thinking develops on a more symbolic level, they start to describe their pain by using more graphic descriptors, such as “terrible, disgusting,” “aching and hurting” (Kortesluoma & Nikkonen, 2006), and “beating or pounding in my head” (Harbeck & Peterson, 1992). Older children tend to include intensifiers when using descriptor words: “really bad;” “pain was radiating…;” “pounding, stabbing, throbbing” (Kortesluoma & Nikkonen, 2006); “horrible; annoying; pin-like; sharp; shooting” (Abu-Saad, 1984a; Harbeck & Peterson, 1992; Savedra, Gibbons, Tesler, Ward, & Wegner, 1982; Wilkie et al., 1990); or “aching; stinging; itching” (Abu-Saad, 1984b; Johnson et al., 2016; Kortesluoma & Nikkonen, 2006; Pölkki, Pietilä, & Rissanen, 1999).
From approximately 8 years of age, children start to think in a more abstract way to describe pain: “Sometimes it is worse and sometimes more like stabbing” (Savedra et al., 1982). Building on these skills, older children (> 10;0) use comparisons (“Like there was a fire inside my head;” “Feels like someone hit it with a sledge hammer”) and define pain as a psychological state based on emotions (“Pain is really upsetting no matter where the pain is;” Kortesluoma & Nikkonen, 2006).
Johnson E, Boshoff K, Bornman J. Scoping review of children’s pain vocabulary: implications for augmentative and alternative communication. Canadian Journal of Speech-Language Pathology and Audiology. 2018;42(1):55-68.
Children’s pain behaviour
“A considerable diversity of actions has been identified as signifying pain in children, including behaviors that could be characterized as verbal (e.g., “asking for help,” “complaining of pain,” and “cursing”), facial activity (e.g., “wincing,” “furrowed brow,” and “widening eyes”), nonverbal vocalizations (e.g., “whimpering,” “crying,” and “moaning”), limb action (e.g., “flailing arms and legs,” “rubbing,” and “protecting/favoring/guarding part of body that hurts”), body action (e.g., “tensing up” and “restless”), physiological manifestations (e.g., “looking pale,” “irregular breathing,” and “shivering torso”), and social behaviors (e.g., “withdrawn,” “hard to console,” and “angry verbalizations”).
Factor analyses yielded three major factors: the “Automatic” factor included items related to facial expression, paralinguistics, and consolability; the “Controlled” factor included items related to intentional movements, verbalizations, and social actions; and the “Ambiguous” factor included items related to voluntary facial expressions.”
Sekhon KK, Fashler SR, Versloot J, Lee S, Craig KD. Children’s behavioral pain cues: Implicit automaticity and control dimensions in observational measures. Pain Research and Management. 2017.
Parents/caregivers
“Parents have well developed, although personal, ways of recognizing and responding to their children’s communication of pain, but also experience uncertainty in their judgments. Parents would benefit from information about the developmental aspects of pain and should be included as active partners in their children’s pain assessment and management.”
Liossi C, Noble G, Franck LS. How parents make sense of their young children’s expressions of everyday pain: a qualitative analysis. European Journal of Pain. 2012;16(8):1166-75.
“Overall, 101 pain incidents were observed, the majority of which evoked low levels of pain and distress, which resolved after 1 min. Pain incidents occurred at a rate of 1.02 incidents/child/hour, with 81% of children experiencing at least one incident, which is higher than previous research with preschoolers and daycare staff. Common parent responses included a range of verbal (reassurance) and nonverbal (staying closer, hugging/kissing child) behaviors. Boys were more likely to not exhibit any protective behaviors. Parents were more likely to pick up older toddlers”.
Noel M, Chambers CT, Parker JA, Aubrey K, Tutelman PR, Morrongiello B, Moore C, McGrath PJ, Yanchar NL, Von Baeyer CL. Boo-boos as the building blocks of pain expression: an observational examination of parental responses to everyday pain in toddlers. Canadian Journal of Pain. 2018;2(1):74-86.
“During the preschool developmental period, parents are instrumental in modelling appropriate pain responding through social learning and modulating their child’s response to pain. Although the literature on parental influences during clinical pain experiences has greatly improved our understanding of social factors in paediatric pain, several avenues of research remain largely unexplored. Specifically, the small number of studies which explored everyday pains spanned a wide time-period, with almost 2 decades between the most recent studies. In this same time period, our understanding of parental influences during clinical pain experiences has advanced significantly, but this evidence does not readily apply to everyday pain experiences. An increased focus should be placed on understanding where children learn about pain and how caregivers respond to common pain incidents in their natural environment.”
O’Sullivan G, McGuire BE, Roche M, Caes L. Where do children learn about pain? The role of caregiver responses to preschoolers’ pain experience within natural settings. Pain. 2021;162(5):1289-94.
On the Exploring Pain: Research and Meaning group on Facebook, Phil Greenfield asks:
“Seeing pain as a ‘thing’ is somewhat inevitable. Pain is so immediate and unpleasant that sufferers naturally want rid of ‘it’. This has spawned a whole raft of of therapeutic models turning out technicians who would claim to be able to remove that ‘thing’ for you.
The experience of pain also has a noun assigned to it (pain) making it even more likely to be seen as a ‘thing’.
The big issue is, how can we uproot that rather persistent problem, and reframe our view of pain as being more akin to love, or grief, or anger, insofar as it has certain sensations associated with it, but that those sensations are not by any means the whole story”.
My response to Phil’s question was (edited):
As I argued in the group here and here, the word ‘pain’, like ‘nausea’, or ‘itch’, is a name of a sensation, but not in the way in which ‘table’ or ‘chair’ are names of furniture. We can point at a table and say that ‘table’ is the name of this (pointing gesture) piece of furniture, but I don’t think we can point at a sensation and say that ‘pain’ is the name of this (pointing gesture) sensation.
I think to say that ‘pain’ is the name of a sensation is to say that there are typical behavioural manifestations of pain, which support statements like ‘Bob is in pain’, and that people who self-report pain are not describing a hidden (Cartesian) object ‘in the mind’, but are signalling to others what is going on with them.
Still, we find it natural to think that pain behaviour is the external sign of a mental object private to the sufferer, which in principle is hidden from observers. In the context of pain underestimation, Kenneth Prkachin writes:
“Evaluating others’ pain is a classic case of decision-making in uncertainty. The difficulty of the task is complicated by the fact that the clinician must try to “look inside” another person. In an ideal world, the clinician would be able to use some kind of “mental dipstick” to slide inside the patient’s consciousness, capture her or his current state, and, on the basis of this reading, recommend further action.
What are the potential sources of underestimation?
A first answer to this question harkens back to the dipstick problem. Because observers do not have direct access to sufferers’ internal experiences, their judgements are reliant on sources of evidence in the sufferer’s behaviour or context. In the setting of most empirical studies, access to that evidence is limited.”
We tend to think that the sole purpose of language is to represent reality; but pain behaviour, including linguistic self-report, does not function to accurately represent a private pain ‘object’. It sounds odd to say, but pain behaviour is not caused by the pain sensation!
Pain behaviour promotes the survival of our species, and is linked with caregiving and care-solicitation; resource allocation and conservation; charity and responsibility toward other members of our big family.
Imagine I see a white rose. The rose is white, not my seeing of it. Right? To think my seeing of the rose is white is to confuse what is perceived, with my perceiving of it. It’s a category mistake.
Now, compare: ‘I feel a burning pain’. To think my feeling of the pain is what burns is, again, to confuse what is perceived, with my perceiving of it.
The pain is what burns, not the feeling of it. Therefore, pain is not a perception.
Question: Whether the pain ‘burns’ or not is down to the perception of the person feeling the pain. It could just as easily be perceived as a ‘stinging’ sensation, a ‘grazing’ sensation, or any other way they wish to describe it. Just because something feels like a burn, doesn’t mean it is, and doesn’t mean it should be treated as such.
Reply: Let me try a different tack: how do you know that you have a pain? Suppose you say, ‘I know I have a pain because I feel (perceive) it’. Makes sense. But ‘I feel it’ means the same as ‘I have it’. Feeling a pain is having a pain. Therefore, ‘I know I am in pain because I feel it’ says no more than ‘I know I have a pain because I have a pain’, which doesn’t explain how you know that you have a pain.
I am arguing that knowledge of pain is not a form of perceptual knowledge (unlike perceiving a white rose). Again: When I feel a pain, there are not two things involved: the pain, and my feeling the pain. There is just the pain. Therefore, pain is not a perception.
Question: Your pain is the perception of it. That is how it works. If you don’t perceive it, it isn’t there. Our reality is constructed from our perceptions and doesn’t exist with them. There is no notion of pain without our perception of it. Pain does not exist independently of our perception of it so I’m not sure what you’re referring to when you say ‘just the pain’.
Reply: I am arguing that pain is not analogous to perceiving a white rose, or to perception of any object in the external environment. Pain is not an ‘object’. Not so long ago, pain was widely identified with the noxious stimulus. Nowadays, some researchers identify pain with a neural activation pattern. Failure to verify pathology can lead to some patients with pain being stigmatised by HCPs.
When I perceive a white rose, there is the rose, and my perceiving it. But ‘pain perception’ is not like this, because feeling a pain is just having a pain (and vice versa). To say that ‘I know I am in pain because I feel it’ just says ‘I know I have a pain because I have a pain’, which doesn’t explain how you know that you have a pain (compare ‘How do you know that you see a rose?’).
The phrase ‘pain perception’ obscures this difference, and understanding this point can help us be a little clearer about the ‘meaning’ of pain.
Question: But aren’t there two (or more things) involved? Say you get a paper cut. There is the cut, with mechanical and chemical nociceptors sending signals to the CNS, and your brain’s perception of the cut and those signals. Your brain perceives a threat and creates pain. There is a rose, and your brain’s perception of the light reflecting off the rose into your eyes, and your brain creates “white”.
Reply: Nice observation! But, my argument doesn’t rely on knowledge of mechanism, but personal experience. That doesn’t limit the clinical relevance of the argument, since clinical decisions are often based on scientific knowledge and personal understanding (‘prior experience’, ‘intuition’, ‘gut feelings’).
Pain is a perception, not a sensation – Mick Thacker – One Thing
The way the sky looks is blue. The colour blue, however, is not an experience. Rather, it is a property of material phenomena. In this case, a property of the sky.
Experiences can be of a blue object, or the colour blue; but to think that experiences can be blue is like thinking that the number two is blue, which is a category mistake.
To make the same point with different examples: – The white rose I see is white, not my seeing of it. – The tightness of my new shoes is not tight, the shoes are. – The bang I hear is loud, not my hearing of it.
The same logic applied to pain experiences: – The pain I feel is piercing, not my feeling it. – The burning of my pain does not burn, the pain does. – The pain I sense is intrusive, not my sensing of it.
I think the view of pain as a perception makes a category mistake: it confuses what is perceived (‘The sky looks blue’; ‘The pain burns’), with a perceiving of it (‘I see the blue sky’; ‘I feel a burning pain’).
The pain is what is painful, not the feeling of it. Therefore, pain is not a perception.
Pain is a material phenomenon of a living organism, a phenomenon characterised by a complex array of distinctive responses and reactions.
Following Wittgenstein, I propose that to feel pain is to have pain – not to feel pain and, in addition, to perceive it. When I feel a pain, there are not two things involved: the pain, and my feeling the pain. Feeling pain is just being in pain.
Imagine two communities. One community predicts the seasonal weather following the science of meteorology. Another community predicts the same through consulting the trusted indigenous oracle. The two communities could be members of the same society, but this is not relevant to the story.
Suppose it turns out that meteorology is far more accurate at forecasting the seasonal weather than the oracle. The community that uses meteorology to predict the weather cultivates a disdain for the oracle community, and criticises it as foolish and irrational.
Should the oracle community therefore abandon its customary oracle practice?
Even if we grant that the oracle community is irrational in adhering to its oracle practice, this does not mean that the community must discontinue the practice, since its adherence could be based on particular needs, priorities, or others factors.
For example, the oracle practice could be influenced by the previous generations’ observations and experimentation, which are highly valued. The oracle forecasts are derived from local experiences and communicated in local languages by the indigenous oracle, who is well-known and trusted in the community. The practice is simple, recognisable, and coherent to the community, compared with the complex and probabilistic nature of scientific forecasts.
In the Last Writings on the Philosophy of Psychology(Volume I), philosopher Ludwig Wittgenstein invites the reader to imagine a tribe unfamiliar with the concept of simulated pain. They
… pity anyone who indicates that he is feeling pain. They are unfamiliar with the suspicious attitude toward expressions of pain. A traveller coming from our culture to theirs frequently thinks that a complaint is exaggerated, indeed, that its only purpose is to generate pity; the natives don’t seem to think that way.
A missionary teaches the people our language; in the process he also educates them and under his tutelage they learn to distinguish between a genuine and a pretended expression of pain … They learn our expression: “to feel pain”, and also “to simulate pain”, and the question is: were they taught a new concept of pain?
Had those people overlooked something, and did the teacher bring something to their attention?
And how could they remain unaware of the difference if sometimes they would complain when they were in pain, and sometimes when they were not? Am I to say that they always thought it was the same thing? – Certainly not. Or am I to say that they didn’t notice the difference? – But why not say: the difference wasn’t important to them? (Last Writings on the Philosophy of Psychology, Volume I, 203-205)
In On Certainty (286), Wittgenstein discusses the possibility that a community could incorporate a different world view into its own practices. Thus, it is possible that the oracle community could use both oracle and meteorological information for weather forecasting. If we assume that agriculture in the community is rainfed and vulnerable to climate extremes and change, meteorological information could help farmers and pastoralists in the community cope with climate variability or adapt to climate change. Still, the community could regard the oracle as superior in relation to specific, important indicators, such as onset of rainfall, or amount of rainfall.
Further, if the oracle community is geographically remote, meteorological weather forecasts may not be downscaled or location-specific, thus less effective in addressing the local needs of community farmers and pastoralists. The forecasts could lack reliability, or capacity in the community to interpret them is limited. Here, the oracle practice would continue to have an essential, or predominant, role in the community.
Presented at the International Network for Research into Psychosocial Adjustment to Long-term Conditions (INRePALC)
1st International Online Networking Event 13th–17th September, 2021
Session Description: Let’s discuss what it means to cope with chronic pain – this is not a data presentation. Instead, I attempt to create a sense of enquiry and self-reflection on how to take the meaning of coping with chronic pain and apply it in the clinic. Thinking about what we do, and what the doing represents in the clinic, can be rewarding.
Presented at the International Network for Research into Psychosocial Adjustment to Long-term Conditions (INRePALC)
1st International Online Networking Event 13th–17th September, 2021
Session Description: Let’s discuss what it means to cope with chronic pain – this is not a data presentation. Instead, I attempt to create a sense of enquiry and self-reflection on how to take the meaning of coping with chronic pain and apply it in the clinic. Thinking about what we do, and what the doing represents in the clinic, can be rewarding.
Lis Dreijer Hammond, Simon van Rysewyk, Chalotte Glintborg, Stephanie Kılınç, Giles Hudson
Abstract
Long-term pain is a common comorbidity for people with acquired brain injury. This chapter explores what it is like to live with those two conditions, focusing on the meaning for the individual. The meaning of pain plays a part in determining people’s emotional reactions and behavioural choices, and it is central for the process of psychosocial adjustment to a life with functional, social, participatory, and emotional challenges. Meaning is also closely linked to the identity changes that typically happen once people are faced with the challenge of living with long-term conditions. The field of positive psychology has contributed valuable insights into this process and the roles of benefit-finding, resilience, and post-traumatic growth are discussed. Two significantly different case stories are used as an illustration of life with acquired brain injury and long-term pain. One case, Julie, illustrates the process of adaptation and the other case, Mark, illustrates the challenge of dealing with pain issues when insight and pain perception has been changed by a frontal lobe injury. In both cases, the meaning of pain is integral to the meaning of brain injury. Neither Julie nor Mark consider themselves to have long-term pain, they live with the long-term impact of their brain injury, where pain is just one aspect. In fact, Mark’s altered pain perception causes him to claim that he feels no pain, yet it is nevertheless a challenge for him. The chapter concludes with clinical recommendations, calling for access to systematic, psychosocial rehabilitation that includes meaning-based approaches. A holistic rehabilitation model is proposed, suggesting that traditional medical and rehabilitation approaches need to happen within the context of psychosocial adjustment and rehabilitation, rather than expecting psychosocial adjustment to happen by itself, as a “by-product” of medical, physical, cognitive, and occupational interventions.
Keywords: chronic, long-term pain, acquired brain injury, meaning, purpose, and identity, psychosocial adjustment and rehabilitation, positive psychology, resilience and benefit-finding, post-traumatic growth
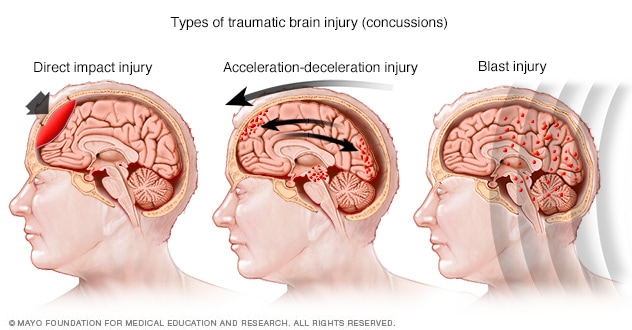
The belief that neonates or infants can feel pain is relatively recent development. Historically, major cardiac surgery was performed in some neonates or infants without anaesthesia, based on the belief that infants had immature nervous systems; therefore, they were incapable of pain, and were fatally vulnerable to the side-effects of anaesthesia. What was standard medical practice in the past is now considered medically unsound and morally unjust. Given that neonates or infants cannot linguistically describe their pain, researchers and clinicians have considered behavioural, physiological, and neurophysiological cues to determine pain in neonates or infants. Pain assessment based on behavioural cues is not an ‘indirect’ means of inferring pain in the neonate and infant because pain experience is not totally separable from its behavioural manifestations. Since pre-linguistic neonates or infants do not possess the concept of pain, in social settings involving pain, the neonate and infant expresses pain only by virtue of a courtesy extended to signs of pain by linguistically competent adults who have already mastered the practice of using ‘pain’. Thus, the aim of this paper is to describe how clinicians and researchers have conceptualised neonatal or infant pain, and what implications these may have in the study of neonatal or infant pain. Craig’s social communications model emphasises how intra- and interpersonal factors surrounding assessment of infant pain influences the caregiver’s ability to decode the behavioural, physiological, and neurophysiological expression of the neonate’s and infant’s pain. Although the neonate’s or infant’s ability to express pain through behavioural signs is an essential aspect of pain assessment, the role of pain detection falls heavily on the caregiver. In some circumstances, such as severe disease acuity, neonates or infants may not have the capacity to respond behaviourally or physiologically to pain. Therefore, it is argued, examining the caregiver’s conceptualisation of the pain is even more important in these circumstances, as it has obvious implications for pain management.
Keywords: neonate, infant, pain, neonatal intensive care unit, pre-linguistic, meaning, concept
How can long-term understanding of established therapies for multiple sclerosis (MS) be harnessed to improve the patient experience? Watch clips from this virtual satellite symposium to:
Learn about the tolerability and possibilities with intramuscular administration of peginterferon beta-1a
Discover new research showing how a different fumarate chemical structure can affect gastrointestinal (GI) tolerability and work productivity while maintaining bioequivalent levels of the circulating active compound mycophenolate mofetil (MMF)
Explore how subcutaneous (SC) administration of natalizumab can reduce the burden of treatment for patients and the healthcare system, a topic of particular relevance during the pandemic
Keep up to date with how long-term safety data is changing the use of established MS therapies
Consider new data and guidelines for MS therapies as they relate to COVID-19
Login to Medthority to view this content, or register an account.
Identify suitable patients with advanced breast cancer to try CDK4/6 inhibitors
Learn the latest CDK4/6 inhibitor survival data from our breast cancer experts
Optimally manage CDK4/6 inhibitor safety in your patients
CDK4/6 inhibitor clinical trials in advanced breast cancer
The cyclin-dependent kinase 4 and 6 inhibitors (CDK4/6 inhibitors) abemaciclib, palbociclib, and ribociclib have been approved by the FDA and the EMA for the treatment of hormone receptor-positive (HR+) and human epidermal growth factor receptor 2 negative (HER2-) advanced breast cancer (ABC).
Login to Medthority to view this content, or register an account.
Presented and recorded at the Australian Pain Society Annual Scientific Meeting, April 2021 virtual event
Topical Session 3C: Meanings of Cancer-Related Pain Tuesday, April 20, 2021 11:15 AM – 12:30 PM
Session Description: Cognitive factors are important determinants of cancer-related pain experience. Simon van Rysewyk describes how cancer-related is particularly sensitive to cognitive factors and describes some common cognitions that people with cancer-related pain have and how they influence patient outcomes. Xiangfeng Xu (Renee) presents on the cultural and social factors that influence cancer pain management of Chinese migrants and what culturally congruent strategies may be implemented to improve their pain outcomes. Melanie Lovell compares levels of suffering in people with cancer-related pain versus non-cancer chronic pain, highlighting differential meanings of existential or spiritual distress and mood dysfunction. Lovell outlines management approaches to cancer pain and suffering that are not responsive to analgesia, such as meaning- or peace-centred therapies.
Session Objectives: At the end of the session, attendees will know: – Common meanings of cancer-related pain and what meanings influence specific patient outcomes – Common meanings of suffering in cancer-related pain and the relationship between these meanings and non-cancer chronic pain experience and mood dysfunction – Effective approaches to diagnosis and management of cancer-related pain symptoms, including interventions based on meaning – Impact of culture on Chinese migrants’ perspectives and responses to cancer pain and recommendations for clinical practice
Presenter Duties Chair: Dr Simon van Rysewyk, University of Tasmania Organiser/Presenter 1: Dr Simon van Rysewyk, University of Tasmania Presenter 2: Dr Renee Xu, University of Sydney Presenter 3: Associate Professor Melanie Lovell, University of Sydney
Slide 2 Human beings are describable in two distinct, but complementary ways: in terms of the way the world is, through scientific descriptions of the causal mechanisms and laws that explain physical things, or, in terms of the way the world seems, through descriptions of personal experiences and meanings.
As a person, I can recognise within myself a perspective or point of view on the world and identify it as belonging to me. Every person has such a unique perspective; this is partly what it means to be a person rather than a physical thing. In contrast, a scientific description of the world does not presuppose any personal point of view. Physical or biological science does not use words like “I”, “here”, or “now”.
Slide 3 The features of personal experience—thought, feeling, speech and action—are amenable to standard scientific explanation as specific changes in the body.
A philosophical assumption held by some neurophysiologists is that a person is identical with his or her body. Person and body are one and the same thing. This assumption is behind the slogan in pain science, “pain is in the brain”.
In terms of personal experience, however, the identity between person and body escapes understanding. For example, when I feel a pain, there is no information or evidence, or nothing that I could discover about my body subsequent to the experience of pain, that could demonstrate it to be false. When I feel a pain, I simply I am in pain.
Slide 4 In person-to-person interactions, we commonly respond to each other as though we are not identical with the human body, but in a compelling sense operating “through” the body, which seems to be a vehicle of thought, emotion, pain or suffering.
We feel that each person we encounter in the world is a unique perspective that is not the body, but the “self”, which is lodged in the face.
Slide 5 Pain is not an action, but a personal experience. Yet, pain reveals itself in those gestures, or expressions, which cannot fail to reveal the person in pain.
People in pain communicate their experience through a range of actions, ranging from self-report, to nonverbal actions, which include paralinguistic vocalisations, bodily activity and facial expressions.
Verbal self-report is mostly voluntary, and relies on reflection and deliberation, whereas nonverbal expression is involuntary and reflexive.
Slide 6 But the involuntary transformations revealed in the face are more meaningful than in other body-parts. This is because body-parts do not have the individuating meaning of the face: the meaning of revealing me, here, now. When I observe another’s pain facial expression, I am not perceiving a physical part of him, as I am when I notice his injured arm or leg. I am meeting him, a real person, who reveals himself in the face.
A person may be perceived by his arm, but not in his arm.
Involuntary facial changes show the person with pain “as he really is”, because he does not fully control them.
We express preference for non-verbal behaviour over verbal behaviour when judging or interpreting the credibility of pain displays.
Slide 7 Pain expressed through the face acquires, for us, an individuality, a personality, that readies us for the human encounter.
Not understanding a face means not seeing where it fits into our gallery of portraits, and therefore not knowing how to properly relate to the person whom it prefigures. One study showed that physicians tended to attribute lower levels of pain to physically attractive patients than physically unattractive patients. Another study found that physically attractive and male patients were perceived as experiencing less pain and disability than physically unattractive and female patients. Finally, in another study, observers judging patient facial pain expressions on video perceived older and less physically attractive patients to be of lower overall functioning.
I can decide to enter into another’s pain expression; or I can decide to remain outside it, as it were, and to see it as a thing apart; perhaps more darkly, as something foreign, or subordinate to my will. How we judge a face may affect the outcomes the patient can achieve.
Slide 8 Pain imposes a significant vulnerability on persons: the vulnerability of a free person who is overwhelmed in his or her body by the presence of pain. This can make the person with pain feel answerable for what he or she experiences. Men who adopt a stoical attitude to their pain are less likely to express pain in the presence of others.
The expression on a face is an offering in the world of mutual responsibilities: it projects into our interpersonal relations a particular person’s “being there”. As soon as I notice pain in another person’s face, my responsibilities are engaged. Facial expressions of pain call on you to respond to me.
The face has this meaning for us because it is the boundary at which the other appears, offering “this person” as one in need of help.
Slide 9 However, expressing pain does not always lead to compassionate reactions, and people are careful about when and with whom they express pain.
Voluntary control of pain through facial actions is normally judged to be an insincere expression of pain, and open to doubt. The controlled pain face is perceived as a mask, which conceals the person lying “behind” it. The expressions on the human face are not always transparent effects of the personal experiences that elicit them, as perhaps they are in non-human mammals. Human beings can deceive through their faces, and children and adults can use the face to fake, and amplify, or suppress, pain.
The capacity to modulate pain expressed through the face has led to difficulty in interpreting the meaning of facially expressed pain. The fidelity with which facial signs mean “pain” is limited to a narrow range of involuntary facial expressions of pain. It is often uncertain whether the presence or absence of information means “pain” or, if they are exaggerated or suppressed consistent with perceived situational demands.
Slide 10 If there is a configuration of facial actions that signals pain, then assessing its presence is amenable to pattern recognition technologies. Substantial progress has been made toward the development of IT-based analysis of pain facial expression.
These systems raise ethical questions about control of patient information. As these IT systems are used in health care settings, informed consent will need to be obtained for collecting and storing patients’ images, but also for the specific purposes for which those images might be analyzed by these systems.
IT systems can store data as a complete facial image or as a facial template. Facial templates are considered biometric data and thus personally identifiable information. The notion that a photo can reveal private health information is relatively new, and privacy regulations and practices are still catching up. Clinicians should advise patients that there may be limited protections for storing and sharing data when using an facial recognition tool.
Immune-mediated inflammatory diseases (IMIDs) are chronic conditions characterised by altered immune regulation causing chronic inflammation in bodily organs or systems. Despite the clinical benefits of biological medicines for IMIDs, the cost of these medicines is relatively high. The high cost of biologics, combined with a stringent regulatory environment in Europe, have created several patient needs, such as access to treatment for IMIDs. As many biologics have now reached patent expiry, several cost-effective biosimilars have been developed and are available for patients with IMIDs.
Biosimilars have enabled lower-cost biologics to enter the market, thereby reducing healthcare spending and releasing budgets that can be reallocated to other disease areas or healthcare services. Cost savings from biosimilars could lead to parity between reimbursement criteria and European clinical guidelines, potentially improving early access to treatments and outcomes in some patients with IMIDs. Improved access can reduce costly surgery and hospitalisations in patients who have benefited from earlier access to biologics.
It is hoped that biosimilars will continue to reduce inequities in the use of biologic medicines for IMIDs and potentially to meet patient needs associated with biologics.
Australian Pain Society Annual Scientific Meeting, April 2021 virtual event
Topical Session 3C: Meanings of Cancer-Related Pain Tuesday, April 20, 2021 11:15 AM – 12:30 PM
Session Description: Cognitive factors are important determinants of cancer-related pain experience. Simon van Rysewyk describes how cancer-related is particularly sensitive to cognitive factors and describes some common cognitions that people with cancer-related pain have and how they influence patient outcomes. Xiangfeng Xu (Renee) presents on the cultural and social factors that influence cancer pain management of Chinese migrants and what culturally congruent strategies may be implemented to improve their pain outcomes. Melanie Lovell compares levels of suffering in people with cancer-related pain versus non-cancer chronic pain, highlighting differential meanings of existential or spiritual distress and mood dysfunction. Lovell outlines management approaches to cancer pain and suffering that are not responsive to analgesia, such as meaning- or peace-centred therapies.
Session Objectives: At the end of the session, attendees will know: – Common meanings of cancer-related pain and what meanings influence specific patient outcomes – Common meanings of suffering in cancer-related pain and the relationship between these meanings and non-cancer chronic pain experience and mood dysfunction – Effective approaches to diagnosis and management of cancer-related pain symptoms, including interventions based on meaning – Impact of culture on Chinese migrants’ perspectives and responses to cancer pain and recommendations for clinical practice
Presenter Duties Chair: Dr Simon van Rysewyk, University of Tasmania Organiser/Presenter 1: Dr Simon van Rysewyk, University of Tasmania Presenter 2: Dr Renee Xu, University of Sydney Presenter 3: Associate Professor Melanie Lovell, University of Sydney
Pain is not an action; yet it reveals itself in those gestures which cannot fail to disclose and to compromise the person with pain.
During pain, body-parts are subject to massive involuntary transformations. But the involuntary transformations revealed in the face are more meaningful than in other body-parts. This is because body-parts do not have the individuating meaning of the face: the meaning of revealing me, here, now. When I observe another’s pain facial expression, I am not perceiving a physical part of him, as I am when I notice his injured arm or leg. I am meeting him, a real person, who reveals himself in the face. A person may be perceived by his arm, but not in his arm. The most meaningful features in displays of pain are the eyes, followed by brows, eyelids, mouth, head, forehead, and then other body-parts. Intentional control of pain through facial movements is normally judged by observers to be an insincere expression of pain, and open to doubt. Thus, involuntary facial changes show the person with pain “as he really is” because he does not fully control them, and observers are more obliged to offer help when movements are most involuntary.
The loss of voluntary control over my body during pain, and its dominion over me, create the compelling sense, for me and for others, of an “incarnate” person. Pain imposes a significant vulnerability on persons: the vulnerability of a free person who is overwhelmed in his or her body by the presence of pain. This can make the person with pain feel answerable for what he or she experiences. The expression on a face is an offering in the world of mutual responsibilities: it projects into our inter-personal relations a particular person’s “being there”. As soon as I notice pain in another person’s face, my responsibilities are engaged. Facial expressions of pain call on you to respond to me. The face has this meaning for us because it is the boundary at which the other appears, offering “this person” as one in need of help. This feature is perhaps at the heart of what it means to treat and monitor pain.
Objective There is a large body of research exploring what it means for a person to live with chronic pain. However, existing research does not help us understand what it means to recover. We aimed to identify qualitative research that explored the experience of living with chronic pain published since 2012 and to understand the process of recovery.
Design A synthesis of qualitative research using meta-ethnography.
Methods We used the seven stages of meta-ethnography. We systematically searched for qualitative research, published since 2012, that explored adults’ experiences of living with, and being treated for, chronic pain. We used constant comparison to distill the essence of ideas into themes and developed a conceptual model.
Results We screened 1,328 titles and included 195 studies. Our conceptual model indicates that validation and reconnection can empower a person with chronic pain to embark on a journey of healing. To embark on this journey requires commitment, energy, and support.
Conclusions The innovation of our study is to conceptualize healing as an ongoing and iterating journey rather than a destination. Health interventions for chronic pain would usefully focus on validating pain through meaningful and acceptable explanations; validating patients by listening to and valuing their stories; encouraging patients to connect with a meaningful sense of self, to be kind to themselves, and to explore new possibilities for the future; and facilitating safe reconnection with the social world. This could make a real difference to people living with chronic pain who are on their own healing journeys.
The question of whether the human fetus experiences pain has received substantial attention in recent times. With the advent of high-definition 4-dimensional ultrasound (4D-US), it is possible to record fetal body and facial expressions.
Objective:
To determine whether human fetuses demonstrate discriminative acute behavioral responses to nociceptive input.
Methods:
This cross-sectional study included 5 fetuses with diaphragmatic hernia with indication of intrauterine surgery (fetoscopic endoluminal tracheal occlusion) and 8 healthy fetuses, who were scanned with 4D-US in 1 of 3 conditions: (1) acute pain group: Fetuses undergoing intrauterine surgery were assessed in the preoperative period during the anesthetic injection into the thigh; (2) control group at rest: Facial expressions at rest were recorded during scheduled ultrasound examinations; and (3) control group acoustic startle: Fetal facial expressions were recorded during acoustic stimulus (500–4000 Hz; 60–115 dB).
Results:
Raters blinded to the fetuses’ groups scored 65 pictures of fetal facial expressions based on the presence of 12 items (facial movements).
(A) Initial items from neonatal facial coding system and 2 supplementary items. 1. Brow lowering. 2. Eyes squeezed shut. 3. Deepening of the nasolabial furrow. 4. Open lips. 5. Horizontal mouth stretch. 6. Vertical mouth stretch. 7. Lip purse. 8. Taut tongue. 9. Tongue protrusion. 10. Chin quiver. 11. Neck deflection. 12. Yawning. (B) Final items from the Fetal-5 Scale. 1. Brow lowering. 2. Eyes squeezed shut. 3. Deepening of the nasolabial furrow. 4. Open lips. 5. Horizontal mouth stretch. 6. Vertical mouth stretch. 7. Neck deflection.
Analyses of redundancy and usefulness excluded 5 items for being of low discrimination capacity (P>0.2). The final version of the pain assessment tool consisted of a total of 7 items: brow lowering/eyes squeezed shut/deepening of the nasolabial furrow/open lips/horizontal mouth stretch/vertical mouth stretch/neck deflection. Odd ratios for a facial expression to be detected in acute pain compared with control conditions ranged from 11 (neck deflection) to 1,400 (horizontal mouth stretch). Using the seven-item final tool, we showed that 5 is the cutoff value discriminating pain from nonpainful startle and rest.
Conclusions:
This study inaugurates the possibility to study pain responses during the intrauterine life, which may have implications for the postoperative management of pain after intrauterine surgical interventions.
Simon van Rysewyk, Melanie Galbraith, John Quintner, Milton Cohen
Although Pain Medicine is a rapidly developing clinical discipline, medical explanations about pain are often unsatisfactory. The problem seems to be with meaning: some people with pain do not find meaning in clinical discussions of pain, and clinicians typically are not looking for it. For patients with pain, biomedical information can be perceived as lacking meaning in relation to their personal experience. By contrast, patient narratives and stories about pain, clinical encounters and therapies, cautionary tales, and common-sense experience seem to offer meaningful and actionable information.
No biomedical explanation of pain, however useful it might be to a pain clinician, could describe the personal meaning or burden of pain to the individual. Traditionally, scientific research has had much to say about the physical nature of pain but much less about pain experience. It seems that one limitation in the ability of clinicians to effectively treat pain or pain-related suffering is an incomplete appreciation of ‘pain experience.’
This special series in Pain Medicine focuses on a pivotal aspect of this problem: how to understand the meaning of pain, for both the patient and the observing clinician.
“One Thing is an experiment. We don’t know where it will lead. But we are clear on one thing: getting these incredible ideas ‘out there’ has amazing potential to help people (people challenged by pain, their loved ones, clinicians, researchers, academics etc!). A brief interview will be released each Friday!“
In 1983, David Copperfield made the Statue of Liberty disappear and reappear on live TV. The illusion was impressive, perhaps astounding, and I think most of us who saw it gazed on in amazement.
In contrast, consider the religious miracle of Jesus turning water into wine at the wedding of Cana. At the wedding, Jesus’ mother told him, “They have no wine.” Jesus replied, “Oh Woman, what has this to do with me? My hour has not yet come.” His mother then said to the servants, “Do whatever he tells you” (John 2:3-5). Jesus ordered the servants to fill containers with water and to draw out some and take it to the chief steward (waiter). After tasting it, without knowing where it came from, the steward remarked to the bridegroom that he had departed from the custom of serving the best wine first by serving it last (John 2:6-10). John adds that: “Jesus did this, the first of his signs, in Cana of Galilee, and it revealed his glory; and his disciples believed in him” (John 2:11).
What makes the Wedding at Cana a religious miracle and not a magical act, like a Copperfield illusion?
One difference must be that some people who witnessed the event immediately understood it as divine expression – “it revealed his glory” – as a result, they “believed in him”. Without noticing this, the event would be astonishing, perhaps strange, but not a religious miracle. Conceived as a magical act, like Copperfield’s Statue of Liberty illusion, people would respond out of incredulity or astonishment, but such responses need not be religious.
The religious significance of the person who commits the miracle is what the event communicates; the significance of the actor is what witnesses are supposed to understand, from a religious perspective, and not everyone will understand. Without this understanding, the Wedding at Cana remains an impressive illusion.
“More and more, we see the value of taking a more patient-centered approach, at every step of the research process,” said Captain Robyn Bent, director of the ongoing Patient-Focused Drug Development (PFDD) initiative, which was established at the US Food and Drug Administration (FDA) in 2012. “In the early stages, that patient input can help researchers understand the impact of the disease and existing treatments, helping us better understand what we need to measure to see if something has worked or not. Once we get to clinical trials, patients can help us understand what aspects of those trials need to be better tailored to fit the needs of the people who will end up participating in those trials. And once a treatment is available, patients can help us understand how to best communicate information to both patients and doctors to facilitate shared decision-making.”
Abstract Pain is a product of our neural networks painstakingly formed through phylogeny and ontogeny. Neural pathways form within neural nets as a result of long term potentiation and other dynamic mechanisms that subserve learning and memory and are modified so therefore form a key part of what Foucault calls “a volume in perpetual disintegration,” constantly reinforcing connections that capture points of experiential association and gradually dismantling networks that are no longer relevant to the organism’s affordances (points of biological significance in a stimulus environment).
Human pain, seen as an experience with a pivotal role in human interactions, and with a number of psychologically inflected varieties and meanings, is therefore not only a neural phenomenon, but also a moral one. It is moral in that it reflects influences from our engagement in a context of human adaptation that is discursive and interpersonal, one that is heavily inscribed by cultural stereotypes and practices that shape who we are and how we understand and give an account of ourselves. To be, in that sense, is to be humanly engaged in the world, including the world of the clinic and its mores whenever and wherever we enter into it.
Unlike experiences mediated by brain pathways designed to transmit and analyse information that tracks and details affairs in the world around us, pain impulses “diffuse” themselves in order to excite reactions and responses such that the primary destination is not the perceptual and analytic areas of the cortex, but areas which convey the impact of the world upon the subjective body and set in motion the body’s highly mediated reaction to contingencies (the touch of the real).
A major feature of complex and mediated cognitive and conative reactions is that, whereas animal drives reflect a simple psychic economy adapted to the natural world, human drives reflect a transformation into terms adapted to a life-world where we tell ourselves and others what is happening and negotiate what should be done to meet the challenges we face.
Gillett G. Neural Plasticity and the Malleability of Pain. In: Meanings of Pain. 2016. (pp. 37-53). Springer, Cham.
Request a pdf copy here. Published in Meanings of Pain, Volume I. Purchase here.
Abstract Mental images are cognitions, which take the form of sensory experiences in the absence of a direct percept. Images can be opposed to verbal thoughts, i.e. cognitions in the form of words. From the perspective of clinical cognition, verbal thoughts and mental images are different phenomena, with mental images having tighter connections to emotion than verbal thoughts. Recently, cognitive psychology research has focused on spontaneous mental imagery, i.e. involuntary intrusions of often vivid mental images that appear in one’s mind. Spontaneous mental imagery is now viewed as an important part of psychopathological processes across psychological disorders, a potential emotional amplifier and a therapeutic target in its own right.
Pain is a personal experience, so exploring and understanding the patient’s thoughts about pain might contribute to therapeutic success and favour personalized care. In the field, thoughts about pain have been mostly studied as verbal thoughts. Yet, a growing literature is investigating thoughts about pain in the form of imagery.
Clinical Implications Studying chronic pain patients’ mental imagery provides unique insight into their personal experience, integrating information about somatosensory perceptions, emotional experience and meanings of pain. The study of imagery in pain also gives insight into possible reinforcing mechanisms of pain, and a basis for a powerful, individualized therapeutic approach through different mental imagery therapy techniques.
This chapter describes current knowledge about mental imagery as intrusive cognitions in the context of pain, considers the neuroscientific investigations that have been undertaken, and discusses the therapeutic potential it yields.
Request a pdf copy here. Published in Meanings of Pain, Volume I. Purchase here.
Abstract Persistent pain is a common health problem and increasingly, qualitative research is being used to explore the impact on daily lived experience. Stigmatisation and “othering” is reported in these studies, and health professionals indicate they struggle to know how best to help this group of people.
In this autoethnography, I provide an account of my life as a clinician, educator, researcher and social media commentator who lives with fibromyalgia. Through this narrative, I consider the social factors influencing my attitudes towards my own pain over time, and the position I hold as a member of many different social groups discussing persistent pain management.
Clinical Implications • People seeking help for their pain are influenced by family habits and attitudes towards healthcare and accepting clinical opinion. • Although persistent pain is common, “othering” or the tendency to see those with persistent pain as different from clinicians (in a negative way) is frequently encountered. This may be inadvertent but results in stigma. • Information about pain mechanisms is insufficient for supporting a new way of living life for people with persistent pain. • People with persistent pain may reject the narratives of people who have learned to live well with their pain, and this can be isolating and difficult to deal with. • There is little research investigating how clinicians advise people of their persistent pain diagnosis, leaving a gap in our understanding of the best way to convey this information. • Researchers who themselves live with persistent pain provide a unique insight into what it is like and may offer new ways for clinicians to carry out their work.
Keywords Othering · Health professional attitudes · Persistent pain · Autoethnography
Abstract First-person narratives of the lived experience of pain, and the meanings of that experience, are uncommon, especially from persons who are not also clinicians or researchers. Yet such narratives could be particularly useful in understanding pain. First-person accounts, stories of pain, can lend unique insights into the lived experience of pain, how individuals make meaning of it, how they come to those meanings, and how those meanings can change over time. Such narratives could lead to new areas of inquiry and explorations of new possible treatment paths.
This chapter provides such a narrative, offering a glimpse into one person’s lived experience of pain and its meanings. It demonstrates how our individual narratives, our stories, help us make sense of our experiences, including pain. It demonstrates how our narratives can change over time as new information and understandings lead to new meanings, and how such changing narratives and meanings can be a part of a therapeutic process that can lead to better outcomes for patients and clinicians alike.
Clinical Implications This chapter provides a first-person account of the lived experience of pain and recovery. It explores the meanings of pain, how they came to be, and how those meanings change over the course of time, from early onset of pain through worsening, unexplained pain to recovery from pain.
Abstract Contemporary pain medicine is necessary to explain pain and to help in its treatment; yet, preference for biomedical explanation of pain in the field has meant that attention to the personal experience of pain and to the meanings of pain experience remain a blind spot in knowledge. Thus, the pain literature includes limited information about the common meanings of living with diabetic peripheral neuropathic pain (DPNP) from the perspective of patients.
The purpose of this chapter is to describe some of the common meanings of pain in patients with DPNP, as currently reported in the literature, how these meanings interact with other common factors in pain experience, including specific negative emotions or moods (depression, anxiety, anger), or the psychosocial context surrounding pain, and to describe available evidence on the effectiveness of cognitive behavioral therapy (CBT) for patients with DPNP. Further quantitative, qualitative or mixed methods research is needed to more fully understand common experiences of pain in patients with DPNP, and the common meanings ascribed to these experiences.
Clinical Implications Pain in patients with DPNP involves a range of threatening pain sensations, including sensations with burning, shooting, tingling, or cramping qualities, and additional more cognitive meanings linked to persistent pain, including a sense that pain disrupts daily life in an intrusive way. Pain affects many aspects of daily experience that are meaningful to patients with DPNP; some describe ongoing physical difficulties, others describe work-related problems or challenges in sexual intimacy. Given the heavy personal burden that DPNP imposes on patients and the considerable challenge of managing the condition pharmacologically, clinical use of non-pharmacological therapies such as CBT for painful diabetic neuropathy might be warranted in individual patients.
Keywords Diabetic peripheral neuropathic pain · Interpretative Phenomenological Analysis (IPA) · Lived experiences · Meaning of pain · Pain experience
Levels of faith and pain intensity Research studies show significant relationships between strong spiritual well-being, increased pain tolerance[1] and an ability to cope with pain.[2]
A recent study demonstrated that spirituality well-being, and faith particularly, as measured by the Functional Assessment of Chronic Illness Therapy – Spiritual Well-Being-Extended scale (FACIT-Sp-Ex), was significantly related to reduced pain intensity in some study participants over a course of pain treatment.[3] What accounts for this relationship? The authors speculated that:
“It may be that a strong element of “faith” is associated with a greater confidence or trust in health professionals and a greater likelihood of following their advice. It is also possible that those with higher levels of “faith” are more likely to improve because they are more likely to engage with a program that seeks to incorporate a spiritual and existential component. It is also possible that they are more eager to please the program providers and report better outcomes. All of these possibilities would need to be explored further and cannot be answered in the present study.”[3]
The quotation suggests that higher levels of faith might be associated with reduced pain intensity in some people with pain.
Forms of faith and pain intensity: a hypothesis A hypothesis is that, in addition to levels of faith, particular forms of faith, or combinations of faith forms, could reduce pain intensity.
So, what forms of faith are there? The following forms are commonly distinguished in philosophy of religion (Table 1).
Faith form
Name in philosophy of religion
A feeling of existential confidence
the ‘purely affective’ model
Knowledge of specific truths, revealed by God
the ‘special knowledge’ model
Belief that God exists
the ‘belief’ model
Believing in (‘trusting in’) God
the ‘trust’ model
Practical commitment beyond the evidence to one’s belief that God exists
the ‘doxastic venture’ model
Hoping the God who saves exists
the ‘hope’ model
Table 1: Common forms of faith identified in philosophy of religion[4]
Scientific study could investigate if some forms of faith are significantly related to reduced pain intensity compared to other forms, or combinations of forms, of faith. These same forms of faith could be used prognostically by clinicians to predict improvements in pain intensity in some patients, or in other outcomes, such as quality of life or pain-related disability. Qualitative research could investigate if patient conceptions of faith accurately map onto faith forms, as identified by philosophers.
Faith beyond religion Can faith exist without commitment to any religion? Tennant wrote that: ‘faith is an outcome of the inborn propensity to self-conservation and self-betterment which is a part of human nature, and is no more a miraculously superadded endowment than is sensation or understanding.’[5] He thinks that ‘much of the belief which underlies knowledge is the outcome of faith which ventures beyond the apprehension and treatment of data to supposition, imagination and creation of ideal objects, and justifies its audacity and irrationality (in accounting them to be also real) by practical actualization.’[5]
If faith exists beyond religion, then people who commit themselves to a view based on a particular interpretation of reality exclusive of the objective verification of the truth, are people of faith. Faith of this kind may be religious without being theistic, as in Buddhism or Taoism. Or, it may be scientific when people propose that reality is no more than what is discoverable by the natural sciences (e.g. ‘scientific atheists’, ‘naturalists’).
Conclusion Study of the interaction between faith and pain could investigate relationships between forms of faith and pain intensity, in addition to other psychosocial outcomes. Such forms span broadly across traditional orthodox religious thesim, relgious non-theism, scientific atheism or naturalism. Interaction between forms and levels of faith, and pain outcomes, is a further possibility. Personal faith could be a useful tool in the clinical armamentarium.
References [1] Lysne CJ, Wachholtz AB. Pain, spirituality, and meaning making: What can we learn from the literature? Religions 2010;2(1):1.
[2] Keefe FJ, Affleck G, Lefebvre J, Underwood L, Caldwell DS, Drew J, et al. Living with rheumatoid arthritis: The role of daily spirituality and daily religious and spiritual coping. J Pain 2001;2(2):101-10.
[3] McCabe R, Murray R, Austin P, Siddall P. Spiritual and existential factors predict pain relief in a pain management program with a meaning-based component. J Pain Manage 2018:11(2):163-170.
Abstract Pain imagery is “like having a picture in your head [of your pain] which may include things you can imagine seeing, hearing or feeling.” Pain imagery may offer a unique insight into a patient’s pain experience. This chapter summarises findings from international pain imagery research in women with endometriosis-associated pain. Endometriosis is a chronic inflammatory condition associated with debilitating pain that affects 5–10% of women of reproductive age worldwide.
Our international research has found that pain imagery is experienced by around half of women suffering from endometriosis-associated pain, and is associated with higher levels of catastrophising, depression, and anxiety. However, coping imagery is also reported, and prevalent, at 30%. Pain imagery in women with endometriosis falls into themes: sensory qualities of pain; loss of power or control; attack (by someone, “something,” or self); pathology or anatomy envisaged; past or future catastrophe; pain as an object; and abstract images. Imagery content may therefore reveal the meanings of pain or endometriosis to these women.
This chapter explores pain imagery content and its personal significance to patients, both for women with endometriosis-associated pain and for patients with other chronic pain conditions. The chapter concludes by discussing the clinical application of imagery, with example patient cases to contextualise the practicalities and therapeutic potential of imagery techniques.
Clinical Implications Pain imagery was reported by half of women with endometriosis-associated pain in our international study and associated with higher levels of catastrophising, depression, and anxiety. Imagery content is extremely varied but can be categorised into themes, which may offer unique insights into each woman’s pain experience. Coping imagery was prevalent at 30%.
We believe imagery techniques may be particularly helpful for women with endometriosis associated pain and discuss these techniques, which should be of interest to professionals involved in pain management.
Happy to announce the first of four papers in the special issue of Pain Medicine – ‘Meaning in the Context of Pain’ – I guest edited with Melanie Galbraith, Dr John Quintner, and Prof Milton Cohen.
Looking for Meaning in Labour Pain: Are Current Pain Measurement Tools Adequate?
Laura Y Whitburn and Lester E Jones
With great advances in understanding the mechanisms of pain, new definitions [1] and classifications [2] have been developed to describe pain conditions…
Australian Pain Society Annual Scientific Meeting, April 2021 virtual event
Topical Session 3C: Meanings of Cancer-Related Pain Tuesday, April 20, 2021 11:15 AM – 12:30 PM
Session Description: Cognitive factors are important determinants of cancer-related pain experience. Simon van Rysewyk describes how cancer-related is particularly sensitive to cognitive factors and describes some common cognitions that people with cancer-related pain have and how they influence patient outcomes. Xiangfeng Xu (Renee) presents on the cultural and social factors that influence cancer pain management of Chinese migrants and what culturally congruent strategies may be implemented to improve their pain outcomes. Melanie Lovell compares levels of suffering in people with cancer-related pain versus non-cancer chronic pain, highlighting differential meanings of existential or spiritual distress and mood dysfunction. Lovell outlines management approaches to cancer pain and suffering that are not responsive to analgesia, such as meaning- or peace-centred therapies.
Session Objectives: At the end of the session, attendees will know: – Common meanings of cancer-related pain and what meanings influence specific patient outcomes – Common meanings of suffering in cancer-related pain and the relationship between these meanings and non-cancer chronic pain experience and mood dysfunction – Effective approaches to diagnosis and management of cancer-related pain symptoms, including interventions based on meaning – Impact of culture on Chinese migrants’ perspectives and responses to cancer pain and recommendations for clinical practice
Presenter Duties Chair: Professor Jane Phillips, University of Technology, Sydney Organiser/Presenter 1: Dr Simon van Rysewyk, University of Tasmania Presenter 2: Dr Renee Xu, University of Sydney Presenter 3: Dr Melanie Lovell, University of Sydney
Meanings of Pain(Springer International Publishing, 2016) was created to advance understanding of pain experience as a bearer of meaning. Progress in modern biomedicine is necessary to explain pain and to aid in its treatment; yet, preference for biomedical explanation of pain in the field has meant that research and clinical attention to the experience of pain and to common factors of pain, such as meaning, as both a clinical topic and a research method, mostly remains a blind spot in knowledge.
Meaningful changes that we notice in others are often subtle and small changes in facial expression, and are similar to features of clinicians that patients find meaningful, such as aspects of clinician demeanour (enthusiasm, positive personality, attentiveness), which are often embodied in subtle facial expressions, gestures, or particular tones of voice (e.g., Gracely et al. 1985). Pain is a personal experience, not an action; yet it displays itself in those actions in which a human person in pain is revealed to observation (Craig et al. 2010). Body-parts are subject to involuntary changes during pain, such as reflexive withdrawal, but in the social transaction of pain, the involuntary changes revealed in the face are more meaningful than in other body-parts (Prkachin et al. 1983; Craig, 2009). This is because body-parts do not have the individuating meaning of the face: the meaning of revealing me, here, now. The expression on a human person’s face is largely determined by involuntary facial actions; yet, it is the living picture of the person that “peers” from it, and hence a concentrated symbol of the “self”. In facial expressions of pain, the face is not a mere bodily part, but the whole person: the self is spread across its surface, and there displayed.
Intentional control of pain through facial actions is normally judged by observers to be an insincere expression of pain, and open to doubt (Hill & Craig, 2002). The controlled pain face is perceived as a mask, which conceals the person lying “behind” it. The expressions on the human face are not always transparent effects of the personal experiences that elicit them, as perhaps they are in nonhuman mammals. Human beings can deceive through their faces, and children and adults can use the face to fake, as well as exaggerate, or suppress, pain (Williams, 2002). It is possible that deception is possible because we do not distinguish a human person from his or her face. Protective acts such as withdrawal reflexes, guarded postures, and disabled behaviour, can communicate pain to sensitive observers (Sullivan, 2008). But when I observe another’s pain face, I am not meeting a physical part of him, as I am when I notice his injured arm or leg. I am meeting him, a real person, who reveals himself in the face as one like me. There are deceiving faces, but not deceiving arms or legs.
Facial expressions of pain call on you to respond to me. As soon as I notice pain in another person, my responsibilities are engaged. I am held to account for it. The face has this meaning for us because it is the boundary at which the other in pain appears, offering “this person” as one in need of help. This feature is perhaps at the heart of what it means to treat pain. Care of persons in pain would be impossible without the assumption that we can commit ourselves through promises, take responsibility now for some event in the future or the past, and enter into obligations that we hold as not transferable to other persons—all of which are perceived in the face.
We may separate pain from its social meaning, and assign to it an impersonal, “bodily” meaning. However, an observation of pain which, whether or not intentionally, focuses exclusively upon the body-parts of another, but which neglects the preliminary changes in the face, as well as in the voice, hands and posture, perhaps is unethical. The failure to recognise the personal existence of the other in pain is therefore an affront, both to him and to oneself. In separating pain from its social meaning, we remove it from the interpersonal world of social relations, which compels us to recognise human beings as persons and sometimes to compromise or risk ourselves for them.
The most meaningful feature in displays of pain is the eyes, followed by brows, eyelids, mouth, head, forehead, and then other body-parts (Prkachin et al. 1983). Although glances are normally voluntary, they participate in the pattern of involuntary social communication where one person in painful distress is “revealed” in his body to the one who observes him. To turn my eyes to you is a voluntary act; but what I receive from you is not anything I voluntarily do. The eye enables the human person in pain to be displayed to another in his body, and in the act of display to call on the observer to intervene on their behalf. The complex transaction of pain involves the voluntary and the involuntary to co-mingle on the surface of the human body. The joining of minds that begins when an expression of pain is answered with a reciprocated response is partly fulfilled in “me seeing you seeing my pain”, which is not the reciprocity of normal cooperation, but of meaning. I believe many patients with pain desire to experience first-hand this more concentrated form of social recognition.
References
Craig KD. A social communications model of pain. Canadian Psychology/Psychologie Canadienne 2009; 50:22-32.
Craig KD et al. Perceiving pain in others: automatic and controlled mechanisms. J Pain 2010; 11(2):101-8.
Hill ML, Craig KD. Detecting deception in pain expressions: The structure of genuine and deceptive facial displays. Pain 2002; 98:135-144.
Prkachin KM et al. Judging nonverbal expressions of pain. Canadian Journal of Behavioural Science/Revue canadienne des sciences du comportement. 1983; 15(4):409.
Sullivan MJL. Toward a biopsychomotor conceptualization of pain. Clin J Pain 2008; 24:281-290.
van Rysewyk S (ed). Meanings of Pain. Springer International Publishing: Switzerland, 2016.
Williams AC. Facial expression of pain: An evolutionary account. Behav Brain Scien 2002; 25:439-488.
Experiencing pain is being in an animal-like state. But, experiencing pain is not knowing that this is pain. I think experiencing pain becomes a state of knowing only if a person is a competent language user.
A consequence of this idea is that pain experience is not always immediately transparent or lucid to the person experiencing it. Odd as it sounds, to be in pain is not to know pain. This challenges the Cartesian philosophy of mind.
Following Derbyshire and Brockman, the fetus or neonate experiences pain, but without understanding or recognition.
—
Emre Ihan asked me: “Do you think learning is a form of recognition? A lot of neonates pull their legs away when nurses and their parents touch their heels, after weeks of heel lancing (heel pricks for blood tests). Could this be an anticipation of pain, and thus recognition that pain is imminent…”
Compare the neonate’s behaviour with a dog walking beside a road with the flow of traffic. The behaviour of the dog conforms to our left-hand drive convention, but it does not do so because it understands that convention.
In the same way, a chicken that stretches its neck and wings as in the mating ritual of the wandering albatross is not stretching its neck because it understands, or has a conception of, this mating pattern.
Point 1. There is behaviour that conforms to a complex pattern.
Point 2. This behaviour is not explained through a conception or understanding of that pattern. The behaviour just accidentally realises part of a complex pattern.
Point 3. The explanation for the behaviour is explained by its relation to the complex patterned whole.
A plausible explanation of the neonate’s behaviour is in terms of the survival value to groups of humans of this form of behavior. These behaviours are performed because they form part of a hard-wired evolutionary pattern, not because the neonate recognises or follows a set of cognitive rules that are an abstract description of the pattern.
Thus, the neonate, like the dog or chicken, does not engage in their patterned behaviour “on purpose.” The neonate does not intend to follow rules or apply social norms.
Developmentally, that skill emerges later when the neonate is a child and learns, if it is fortunate enough, the concept of pain.
Volume III Topic: Meanings of pain in vulnerable or special patient groups
Series Editor: Dr Simon van Rysewyk Publisher: Springer
The Meanings of Pain book series describes how the meaning of pain changes pain experience – and people – over time.
Pain in the moment is experienced as immediately distressing or unpleasant. If pain persists over time, more complex meanings about the long-term consequences, or burden of pain, can develop. These meanings can include existential meanings such as despair or loneliness that focus on the person with pain, rather than pain itself.
Meanings of Pain offers a vocabulary of language about pain and meaning. An objective of the series is to stimulate self-reflection on how to use information about meaning in clinical and non-clinical pain settings. The book series is intended for people with pain, family members or caregivers of people with pain, clinicians, researchers, advocates, and policy makers.
Although chronic pain can affect anyone, there are some groups of people for whom particular clinical support and understanding is urgently needed. This applies to “vulnerable” or “special” groups of people and to the question of what pain means to them.
Volume III focuses on describing the meanings of pain in groups of “vulnerable” or “special” people, such as:
Infants or children
Women
Older adults
People with a physical or intellectual disability
People with a brain injury
People diagnosed with a disease
Veterans
Athletes
Workers
Addicts
People with mental illness or mental disorders
Homeless people
People in rural or remote communities
People in multicultural communities
Indigenous peoples
Invited chapter types The editor Dr Simon van Rysewyk invites contributions for Volume III on the meanings of pain in vulnerable or special patient groups. The following manuscript types will be considered:
Original Research (e.g., original clinical, translational, or theoretical research)
Authors interested in submitting a chapter for publication in Volume III are invited to submit a 350-word Abstract, which includes the name and contact information of the corresponding author, to:
Dr Simon van Rysewyk simon.vanrysewyk@utas.edu.au
Abstract Deadline: closed
“It is my opinion that this … work will stand as the definitive reference work in this field. I believe it will enrich the professional and personal lives of health care providers, researchers and people who have persistent pain and their family members. The combination of framework chapters with chapters devoted to analysing the lived experience of pain conditions gives the requisite breadth and depth to the subject.” – Dr Marc A. Russo, MBBS DA(UK) FANZCA FFPMANZCA, Newcastle, Australia, from the Foreword in Volume II
Australian Pain Society Annual Scientific Meeting 2020 Hobart Tasmania
Topical Session Tuesday, April 7, 2020, 3.30-5.00pm
Session Description: Cognitive factors are important determinants of cancer-related pain experience. Simon van Rysewyk describes some common meanings and beliefs that people have about cancer, illness, and pain, and the consequences these meanings have in relation to common help-seeking behaviours or coping strategies people choose to adopt. Suffering is a cognitive and emotional response to recurrent perceived losses experienced in some people with cancer. Megan Best presents on the challenges in assessing people with cancer-related suffering and the relationship of suffering to cancer-related pain. Melanie Lovell compares levels of suffering in people with cancer-related pain versus non-cancer chronic pain, highlighting differential meanings of existential or spiritual distress and mood dysfunction. Best and Lovell outline management approaches to cancer pain and suffering that are not responsive to analgesia, such as meaning- or peace-centred therapies.
Session Objectives At the end of the session, attendees will know: – Common meanings of cancer-related pain and how people apply these meanings to cope with their pain – Common meanings of suffering in cancer-related pain and the relationship between these meanings and non-cancer chronic pain experience and mood dysfunction – Effective approaches to diagnosis and management of cancer-related pain symptoms, including interventions based on meaning
Presenter Duties Chair: Professor Jane Phillips, University of Technology, Sydney Organiser/Presenter 1: Dr Simon van Rysewyk, University of Tasmania Presenter 2: Dr Megan Best, University of Sydney Presenter 3: Associate Professor Melanie Lovell, University of Sydney
As organisms, human beings interact with the world and each other through causal mechanisms that control us and every other physical thing. As persons, we act in the world through our thoughts, emotions, attitudes, or desires.
Accordingly, human beings are describable in two distinct, but complementary ways: in terms of the way the world is, through scientific descriptions of the causal mechanisms and laws that explain physical things, or, in terms of the way the world seems, through descriptions of personal experiences and meanings.
One or the other way of describing human beings comes into focus depending on the questions we ask about ourselves or the world. The features of personal experience—thought, feeling, speech and action—are amenable to standard scientific explanation as specific changes in the body. Traditionally, scientific research has had much to say about the physical nature of pain, but much less about the personal experience or meaning of pain. Indeed, the meaning of pain remains a blind spot in knowledge.
A description of a human being as a person means that there is a way of understanding of human beings in which personal experience and meaning, rather than physical causation alone, is needed to answer the question, “What is happening?”
Human persons can distinguish between how things are in the world and how things seem to me. I can recognise within myself a perspective or point of view on the world and identify it as belonging to me. Every person has such a unique perspective; this is partly what it means to be a person rather than a physical thing. In contrast, a scientific description of the world does not presuppose any personal point of view. Physical science does not use words like “I”, “here,” or “now”. Does this mean that “persons” are unobservable to standard quantitative science?
Possibly. Imagine a complete explanation of pain according to the final neurophysiology of pain—whatever it turns out to be. Such an explanation of pain would, to put it very crudely, accurately map specific neurophysiological changes in physical parts in the living human organism and all their true causal interactions across time. However invaluable such an explanation would be to pain medicine, it could not describe the way pain seems to the person who experiences it, for which of the physical objects described in this explanation is me with pain, here, now? Immediate pain always seems a certain way to persons, and this “seeming” determines the experience of the person with pain. In describing personal pain, human beings use language with other meanings than the language used in neurophysiology. The final neurophysiological explanation of pain therefore could explain only one dimension of pain in human beings—the physical dimension—in language that could not capture the personal experience, burden, or meaning of pain.
A philosophical assumption of neurophysiology is that a person is identical with his or her body. Person and body are one and the same thing. In terms of personal experience, however, the identity between person and body escapes personal understanding. For example, when I feel a pain, there is no information or evidence, or nothing that I could discover about my body subsequent to the experience of pain, that could demonstrate it to be false. When I feel a pain, I simply know that I am in pain.
In person to person interactions, we commonly respond to each other as though we are not identical with the human body, but in a compelling sense operating “through” the body, which seems to be a vehicle of thought, emotion, pain or suffering. We feel that each person we encounter in the world is a unique perspective that is not the body, but the “self”, which peers out through the face. The human face is the social instrument of persons. In seeking to understand you, or adjust how the world or your experience seems to you, I interact with you through your embodied perspective.
In pain experience, it is my loss of personal control over my body, and its dominion over me, that create the compelling sense, for me and for others, of an “incarnate” person. Pain imposes a significant vulnerability on persons: the vulnerability of a free person who is overwhelmed in his or her body by the presence of pain. This can make the person, and the person’s significant others, feel answerable for what he or she experiences.